Information for patients
This leaflet can be made available in other formats including large print, CD and Braille and in languages other than English, upon request.
What is a pneumothorax?
A pneumothorax is also known as a collapsed lung. It is a condition when air has leaked out from the lung in to the chest cavity and chest wall. This causes the lung to collapse down and peel away from the inside of the chest.
What causes a pneumothorax?
There are different types of pneumothorax:
- Primary pneumothorax: This is when someone has developed as pneumothorax who doesn’t have any known lung problems. Usually the air has leaked from a blister or bleb on the surface of the lung which has been present from birth.
- Secondary pneumothorax: This is the term applied when a patient has a known underlying lung condition which predisposes them to this problem. For example, Chronic Obstructive Pulmonary Disease (COPD) or emphysema.
- Traumatic pneumothorax: This refers to when someone has suffered an injury to the chest wall such as a fall which has caused damage to the surface of the lung.
- Iatrogenic pneumothorax: Describes when a pneumothorax has happened after a medical procedure. This can include lung biopsies, camera tests and procedures to remove the fluid from the lung.
A pneumothorax can happen more commonly in smokers. There are rarer genetic lung conditions which can predispose people to lung damage who can develop a pneumothorax because of this.
What symptoms might I get?
The most common symptoms are sudden shortness of breath and chest pain (which may be sharp and worse with coughing and breathing).
You may also experience a dry cough.
If air has leaked out into the muscles and skin in your chest wall you may notice a swelling and a “bubble wrap” sensation if you press on your chest.
Occasionally if the leak of air has been very large you may feel faint or light headed.
How is it diagnosed?
The most important investigation to diagnose a pneumothorax is a chest X-ray. This is usually enough in most cases to show the collapsed lung.
Sometimes a CT scan, which is a three dimensional X-ray, may be arranged for a more detailed assessment of the pneumothorax, or if the team aren’t confident based on your chest X-ray.
You may also have other tests in addition to X-rays. These can include blood tests and heart tracings (ECGs), especially if you have been very unwell. This is to look for other causes and have an idea of how the pneumothorax is affecting the rest of your body.
If the pneumothorax has made you very unwell when you were first admitted, the doctors may have had to do a procedure to relieve it before you had an X-ray or any other tests. This is very rare.
What treatment might I have?
The treatment for your pneumothorax would depend on how large it was and also how unwell it made you.
A small pneumothorax may not need any treatment. In this case the lung heals itself and gradually reabsorbs the air that has leaked out. This generally takes 1 to 2 weeks. In this situation you may be admitted to hospital overnight and have another chest X-ray the following morning to make sure that no more air has leaked out.
You will normally be brought back for further X-rays as an outpatient until your lung has returned to normal.
A larger pneumothorax may need a procedure to remove the air and allow the lung to re-inflate. These can include:
Pleural Vent
This a small chest drain which is inserted in the upper part of the front of your chest wall. It allows the air to escape from your chest. It is used in patients whose pneumothorax is expected to take 1 to 3 days to heal.
It is inserted under local anaesthetic and you can return home shortly after it has been put in. You will need to return to clinic usually every day or two to check that things are getting back to normal
Pleural aspiration
This is a procedure where a small needle or plastic tube is inserted between the ribs of your upper chest wall and the air removed using a syringe.
This is a fairly simple procedure, done under local anaesthetic. It is normally performed when a patient has had a pneumothorax in a situation that the lung is expected to heal very quickly. This may happen after a procedure such as a lung biopsy.
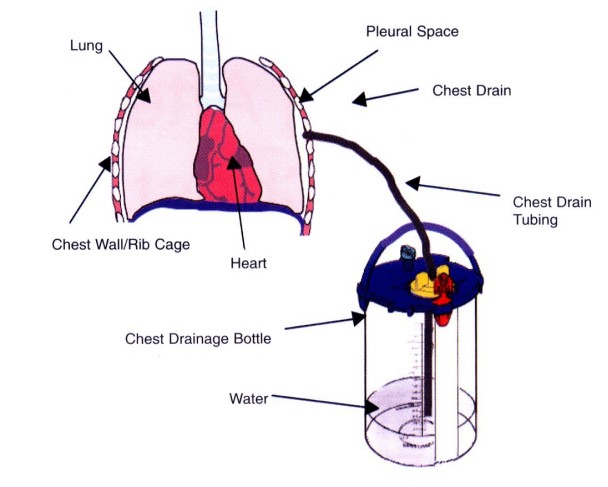
Chest drain (Intercostal drain)
This is a procedure where a small plastic tube (similar size to a regular drinking straw) is inserted between the ribs. This is usually inserted in your armpit or back. This tube usually stays in place for at least 24 to 48 hours.
It is attached to a small plastic fluid filled container which sits on the floor next to your bed. This allows the air to bubble out without going back into your chest. The chest drain is removed when the air has stopped bubbling out of the drain and the team are happy that the lung has healed.
Very occasionally the tear in the lung does not heal. In this situation we may apply ‘suction’ to the drain to draw air out. If this still does not heal the lung, we may ask the chest surgeons to consider doing an operation to try and find the damage to the lung and repair it.
Could this happen again?
About 1 in 3 people who have had a pneumothorax will have another within 12 months.
This is more likely if you continue to smoke if or if you have an underlying condition.
What can I do to help myself get better?
If you smoke, the best thing you can do is to stop or cut down.
While you are getting better, we do encourage gentle exercise such as walking. You will feel more easily breathless than usual for you.
We ask you to avoid strenuous exercise and lifting heavy objects for at least 4 weeks.
What is it happens again?
If your symptoms come back, we ask you to attend your nearest A&E department. If you are unwell please ring 999 and explain that you have had a pneumothorax recently and that you are feeling the same symptoms. If you are well enough to make your own way to hospital, we ask you not to drive but to get someone else to.
If your pneumothorax has come back, the treatment is likely to be the same initially. Once you have recovered we will refer you to a chest surgeon. They will consider an operation to look inside your chest and perform a procedure to stop this happening again.
We only refer you for this if you have had at least two collapsed lungs on the same side of your chest or if both of your lungs have collapsed at different times.
Will I need any other tests or follow up?
You will usually be asked to come back to the chest clinic, especially if you have had a small pneumothorax which hasn’t had any treatment.
If your team suspect there may be an underlying condition that has caused this pneumothorax, they may also ask you to have blood tests, CT scans and breathing tests. They will arrange for you to come to clinic to review the results.
What other things do I need to think about?
You should not fly while your lung is healing. Most airplane companies will allow you to fly 2 weeks after a chest X-ray which has shown that the pneumothorax has healed.
We are more conservative and would advise you to wait at least 6 weeks and preferably 3 months before you consider flying.
If you have had a pneumothorax, we advise you never to take up scuba diving as a hobby, unless you have had surgery to repair the damaged bit of lung.
You are unlikely to be offered employment as a professional diver if you have had a pneumothorax unless you have had a definitive operation to your chest to ensure that it cannot happen again.
Where can I find more information?
The British Lung Foundation
Website: https://www.blf.org.uk/support-for-you/pneumothorax
Contact numbers
Lung Health
Telephone: 01642 624270
Department of Respiratory Medicine
Monday to Friday
09:00 a.m. to 05:00 p.m.
Telephone: 01642 624936
Emergency Department
24 hours a day, 7 days a week
Telephone: 01642 382899
Comments, concerns, compliments or complaints
Patient Experience Team (PET)
We are continually trying to improve the services we provide. We want to know what we’re doing well or if there’s anything which we can improve, that’s why the Patient Experience Team (PET) is here to help. Our Patient Experience Team is here to try to resolve your concerns as quickly as possible. The office is based on the ground floor at the University Hospital of North Tees if you wish to discuss concerns in person. If you would like to contact or request a copy of our PET leaflet, please contact:
Telephone: 01642 624719
Freephone: 0800 092 0084
Opening hours: Monday to Friday, 9:30am to 4:00pm
Email: [email protected]
Out of hours
Out of hours if you wish to speak to a senior member of Trust staff, please contact the hospital switchboard who will bleep the appropriate person.
Telephone: 01642 617617
Data protection and use of patient information
The Trust has developed Data Protection policies in accordance with Data Protection Legislation (UK General Data Protection Regulations and Data Protection Act 2018) and the Freedom of Information Act 2000. All of our staff respect these policies and confidentiality is adhered to at all times. If you require further information on how we process your information please see our Privacy Notices.
Telephone: 01642 383551
Email: [email protected]
Privacy NoticesLeaflet feedback
This leaflet has been produced in partnership with patients and carers. All patient leaflets are regularly reviewed, and any suggestions you have as to how it may be improved are extremely valuable. Please write to the Clinical Governance team, North Tees and Hartlepool NHS Foundation Trust, University Hospital of North Tees, TS19 8PE or:
Email: [email protected]
Leaflet Reference: PIL1217 – Version 02
Date for Review: 17/12/2027