Information for patients
This leaflet can be made available in other formats including large print, CD and Braille and in languages other than English, upon request.
Introduction
This leaflet will explain what Endoscopic Submucosal Dissection (ESD) is and when it is required. ESD involves removing growths (polyps) from the wall of your bowel, using an endoscope and an electrically heated knife.
Such growths in the bowel may be cancerous, potentially cancerous, or harmless (benign).
Treatment usually involves removal of the growth, together with a small area of tissue around the growth.
This procedure is used for large growths that are difficult or impossible to remove using other techniques.
The procedure follows advice from the National Institute for Health and Care Excellence (NICE), making the procedure as safe and efficient as possible.
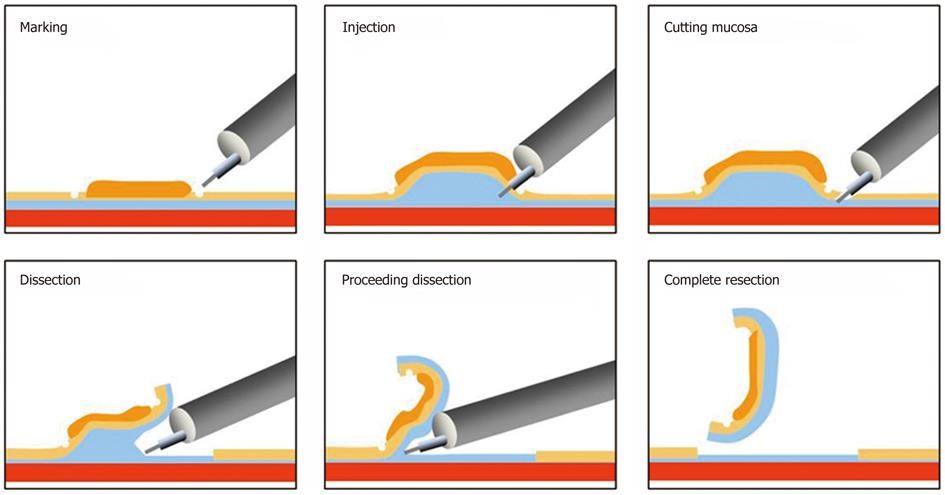
What does the procedure involve?
- The procedure will be performed either under general anaesthetic or deep sedation. If your procedure is predicted to be short, simple conscious sedation may be used (you will have discussed this with the team beforehand).
- An endoscope (flexible camera) will be used to view your bowel wall and access the irregular area (polyp).
- Once the polyp has been located, fluid will be injected underneath it to lift the polyp away from the bowel wall muscle layers, making it easier and safer to remove.
- The polyp is then carefully resected (cut out) from the bowel wall using a special diathermy (heat treated) knife.
What are the benefits of ESD?
Polyps in the colon carry a risk of turning cancerous in the future. Not all polyps will become cancerous but if they do it usually takes several years to happen. Some larger polyps can already contain early cancer cells.
The main benefit of this procedure is to avoid you having to undergo major surgery. Removal of the polyp in one piece allows us to examine it in detail under a microscope, giving the best opportunity to know if it has been fully removed. Removing the polyp in one piece also reduces the chance of it growing back in the future.
What care will I need after the procedure?
ESD is planned as a day case procedure. This means that if all goes well and depending on the time of your appointment, you may go home after the anaesthetic or sedation has worn off.
You will be asked to look for symptoms such as blood in your stools (poo) and any fever or pain for 2 to 3 weeks after the procedure. If you do get these symptoms, you should return to hospital for examination.
How will I feel after the procedure?
Due to the sedatives or anaesthetic drugs you have been given, you may feel sleepy for a few hours following the procedure.
For a few days after the procedure, you may experience:
- mild discomfort (soreness)
- mucus discharge from your bottom
- minor bleeding
- changes to your bowel habits (constipation/diarrhoea).
This is a normal part of your healing process and may vary depending on the area the growth was in.
What if something goes wrong?
If you experience any of the symptoms described (blood, fever, severe pain), we may need to keep you in hospital as an inpatient.
This usually involves close observation of your vital signs, sometimes a repeat camera examination (e.g. to stop bleeding), a scan and occasionally open surgery to repair your bowel in case of a puncture (“perforation”).
How well does the procedure work?
Studies show that growth removal rates, where the growth was removed in 1 piece, were higher for lesions treated with ESD than with endoscopic mucosal resection (EMR). Research shows that ESD achieves single piece resection in 8-9 out of 10 of cases, with clear margins (“cure”) achieved in approximately 7 out of 10 cases.1
What are the risks and potential complications involved?
The main risks are:
Bleeding. Bleeding may occur in about 1 in 20 patients.
Sometimes bleeding occurs during the test, but it can also occur up to 14 days after the procedure. If bleeding does occur, it often stops on its own. However, very occasionally it requires a blood transfusion or further endoscopies. Very rarely, emergency surgery may be needed to stop it.
Perforation. This means a tear in the bowel wall. For ESD, this occurs about 5 to 6 in every 100 patients.7, 8 If the perforation occurs during the procedure, it can usually be managed using endoscopic clips. You may need to stay in hospital. Treatment may also include intravenous antibiotics and fluids.
In rare cases an emergency surgical operation is required. As with any bowel operation, a stoma (bag on your abdomen) may be required, although this would usually be temporary. The operation may be “open” or “keyhole” (laparoscopic) surgery.
Any emergency operation may be life threatening (lead to death) or alter your future quality of life.
Interrupting your blood thinning medication: If you take any drugs to thin your blood, you will be asked to stop these temporarily prior to ESD. If you usually take Warfarin, we may arrange for you to have daily injections of heparin instead. This will help to reduce the risk of bleeding.
Most patients do not develop problems while they are not taking their blood thinning medication, however there is an increased risk of developing blood clots or having a stroke during this time. This is something you may wish to discuss with the endoscopist prior to your procedure.
Other risks include:
- Causing a cancerous lesion to spread (potentially becoming incurable).
- There is a chance that due to complications, the growth may not be able to be removed in one piece.
- There is also a chance that regrowth (recurrence) may occur months after the procedure.
- Extra surgery may be needed after ESD, if analysis under the microscope suggests deep cancerous invasion of the bowel wall.1, 2
- Regrowth (“recurrence”) of polyps removed using ESD in the following 12 months is also rare.1, 3
Are there alternative procedures to ESD?
Yes, the main alternative procedures include:
Endoscopic Mucosal Resection or EMR
This procedure often removes growths in more than one piece, making it difficult to analyse under a microscope. It is often uncertain as to whether the polyp has been completely removed. Follow up checks are often needed to ensure regrowth doesn’t occur. Risks of EMR are similar to ESD (bleeding and perforation) although the likelihood of such a complication occurring is lower than with ESD.
Transanal Endoscopic Surgery (for lesions or polyps in the rectum)
This procedure requires general anaesthesia and is performed through the anus. It can only be used for growths in the rectum. Research shows it is similar to ESD in terms of safety and efficiency, but leads to a longer hospital stay.5, 6
Other options include open surgery (cutting of the skin and tissues) and keyhole surgery (laparoscopic) which is minimally invasive and uses small incisions. This is usually means a longer recovery and may carry greater risks.
Do nothing:
Alternatively, you may opt not to have the lesion or polyp removed. The risks of this option are that the polyp will continue to grow and develop into cancer in the future (if not already cancer). There is also a risk of the polyp causing symptoms if left untreated. This decision must be carefully considered after discussion with your consultant.
What does this information mean for me?
Your doctor or nurse specialist will explain the procedure in full detail as well as the risks and benefits involved. You will be given the opportunity to ask any further questions.
References
- Thorlacius H, Ronnow CF, Toth E. European experience of colorectal endoscopic submucosal dissection: a systematic
review of clinical efficacy and safety. Acta Oncol 2019;58:S10-s14.
Available at: https://www.tandfonline.com/doi/full/10.1080/0284186X.2019.1568547
- NICE. Endoscopic Submucosal dissection of lower gastrointestinal lesion. National Institute for Health and Clinical Excellence 2010.
Available at: https://www.nice.org.uk/guidance/ipg335
- Patel N, Patel K, Ashrafian H, et al. Colorectal endoscopic submucosal dissection: Systematic review of mid-term clinical outcomes. Dig Endosc 2016;28:405-416.
Available at: https://onlinelibrary.wiley.com/doi/abs/10.1111/den.12597
- De Ceglie A, Hassan C, Mangiavillano B, et al. Endoscopic mucosal resection and endoscopic submucosal dissection for colorectal lesions: A systematic review. Crit Rev Oncol Hematol 2016;104:138-55.
Available at: https://www.sciencedirect.com/science/article/abs/pii/S104084281630141X
- Sagae VMT, Ribeiro IB. Endoscopic submucosal dissection versus transanal endoscopic surgery for the treatment of early rectal tumor: a systematic review and meta-analysis. 2019.
Available at: https://link.springer.com/article/10.1007/s00464-019-07271-2
- McCarty TR, Bazarbashi AN, Hathorn KE, et al. Endoscopic submucosal dissection (ESD) versus transanal endoscopic microsurgery (TEM) for treatment of rectal tumors: a comparative systematic review and meta-analysis. 2019
Available at: https://link.springer.com/article/10.1007/s00464-019-06945-1
- Landin, M.D. and Guerrón, A.D., 2020. Endoscopic mucosal resection and endoscopic submucosal dissection. Surgical Clinics, 100(6), pp.1069-1078.
Available at: https://www.surgical.theclinics.com/article/S0039-6109(20)30082-7/abstract
- Pimentel-Nunez et al. Endoscopic submucosal dissection for superficial gastrointestinal lesions: European Society of Gastrointestinal Endoscopy (ESGE) Guideline – Update 2022
Available at: https://www.thieme-connect.com/products/ejournals/html/10.1055/a-1811-7025
Further information is also available from the National Institute of Health and Care Excellence website
https://www.nice.org.uk/guidance/IPG335
Comments, concerns, compliments or complaints
Patient Experience Team (PET)
We are continually trying to improve the services we provide. We want to know what we’re doing well or if there’s anything which we can improve, that’s why the Patient Experience Team (PET) is here to help. Our Patient Experience Team is here to try to resolve your concerns as quickly as possible. The office is based on the ground floor at the University Hospital of North Tees if you wish to discuss concerns in person. If you would like to contact or request a copy of our PET leaflet, please contact:
Telephone: 01642 624719
Freephone: 0800 092 0084
Opening hours: Monday to Friday, 9:30am to 4:00pm
Email: [email protected]
Out of hours
Out of hours if you wish to speak to a senior member of Trust staff, please contact the hospital switchboard who will bleep the appropriate person.
Telephone: 01642 617617
Data protection and use of patient information
The Trust has developed Data Protection policies in accordance with Data Protection Legislation (UK General Data Protection Regulations and Data Protection Act 2018) and the Freedom of Information Act 2000. All of our staff respect these policies and confidentiality is adhered to at all times. If you require further information on how we process your information please see our Privacy Notices.
Telephone: 01642 383551
Email: [email protected]
Privacy NoticesLeaflet feedback
This leaflet has been produced in partnership with patients and carers. All patient leaflets are regularly reviewed, and any suggestions you have as to how it may be improved are extremely valuable. Please write to the Clinical Governance team, North Tees and Hartlepool NHS Foundation Trust, University Hospital of North Tees, TS19 8PE or:
Email: [email protected]
Leaflet reference: PIL1210
Date for Review: March 2027